
Reconnect with Quality Care
Board Certified in Otolaryngology – Head & Neck Surgery (1987)
Fellow in American Academy of Otolaryngic Allergy (1995)
Let’s begin the discussion with, “How do I know I have a hearing problem?” Well, in each of my ENT exam rooms there is a poster that is titled, ‘How is your hearing?’
This is how the initial office visit starts – in fact, both the Audiologist completing your hearing test (audiogram) and I will continue to ask about situations that seem to be associated with your hearing difficulties. This is how we get an idea of how to help you improve your hearing… more later. We will also ask about a variety of ‘risk factors’ for hearing loss… some of these are pretty obvious:
- Noise Exposure…
work related noise exposure, use of guns without hearing protection, exposure
to loud music. (Parents… if you can hear
the music from your kid’s headphones or ear buds – it’s too loud!!!) This may now be the #1 cause of hearing loss. - Age… 30% of us
over the age of 60 will have hearing loss… and it gets worse as we all get
older! - Family History…
your parents give you both the good and the bad! - Medications…
certain antibiotics and cancer (chemotherapy) medications are associated with
the loss of the inner ear ‘hair cells’ (see below). - Health Conditions… acute illnesses such as severe infections or trauma may cause hearing
loss. Poorly controlled high blood
pressure, diabetes, and high cholesterol are chronic health conditions that create
a higher risk of hearing loss. - Outer Ear
canal conditions such as recurring ear wax impactions and chronic eczema of the
ear canal skin create recurring problems with the sound wave passing to the ear
drum. (See ear diagram) - Middle Ear
infections prevent the sound wave from passing efficiently from the ear drum,
through the three hearing bones, and into the inner ear. (See ear diagram) - Inner Ear conditions
such as viral infections that cause the sudden loss of hearing, certain
autoimmune diseases, an inner ear condition called Meniere’s Syndrome that is
associated with progressive hearing loss and episodes of a severe spinning
sensation (vertigo) – all can cause permanent loss of the ‘hair cells’ in the
inner ear. (See ear diagram) - ‘Brain Problems’…
one way to think about this possible cause of hearing problems is that the ear
takes the energy of sound waves and creates nerve energy for the brain to use –
but its really the brain that ‘hears and understands’ the information present
in the sound wave of speech, music, a car horn, or doorbell. This is such an important health problem that
I’ve included a separate discussion at the end of this page… see ‘Hearing and
the Brain’.
Following this initial discussion, I will examine your outer ear (auricle), ear canal (auditory canal) and eardrum (tympanic membrane). Many times I will need to use an operating microscope to clean your ear canal of ear wax (cerumen) before the Audiologist completes the hearing test (audiogram).
After we: 1) discuss how your hearing seems to be affecting your day-to-day activities; 2) discuss potential risk factors for your hearing difficulties; and 3) examine your ear, I will have you walk over to the Southwestern Hearing Center to have the Audiologist complete a comprehensive hearing test or AUDIOGRAM.
However, before I move into a discussion of how hearing is measured with an audiogram, I think I should describe the basics of how hearing works.
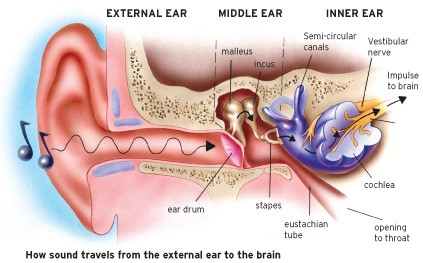
- The information of
sound and speech travels in the energy of a soundwave. - The soundwave
travels down your auditory canal to the eardrum (tympanic membrane) where the
energy of the soundwave moves the eardrum back and forth. - The movement of
the eardrum is then ‘concentrated’ by movement of the hearing bones (malleus,
incus, stapes) down to the inner ear. - Inside the inner
ear, the energy within the movement of the hearing bones stimulates the hair
cells of the inner ear (cochlea). These hair cells have the ability to transform
the energy in the soundwave into nerve energy that the brain uses for hearing.
Hearing Test or Audiogram
A couple of words about hearing tests or audiograms. The actual hearing test is conducted by an Audiologist. The Audiologist is a healthcare professional with doctorate level degree in disorders of hearing and balance. The Audiologist’s role in hearing and balance care may include:
- assisting in the
diagnosis of your hearing and/or balance problem by completing and interpreting
many of the diagnostic studies; - counseling
patients on communication strategies that may be helpful in dealing with their
hearing loss; - treating hearing
loss by helping the patient use and manage the many hearing aid technologies
available.
For adults, the audiogram is a graph representing individual Frequencies (cycles of sound/second) of sound that a human uses for speech compared to the Hearing Level (decibels) of how loud the noise or speech has to be for the patient to hear the sound. (Note: there other kinds of audiograms the Audiologist will use for infants and children younger than 5 years of age.) In order to understand the information on an audiogram, let’s look at an ‘Audiogram of Familiar Sounds’:
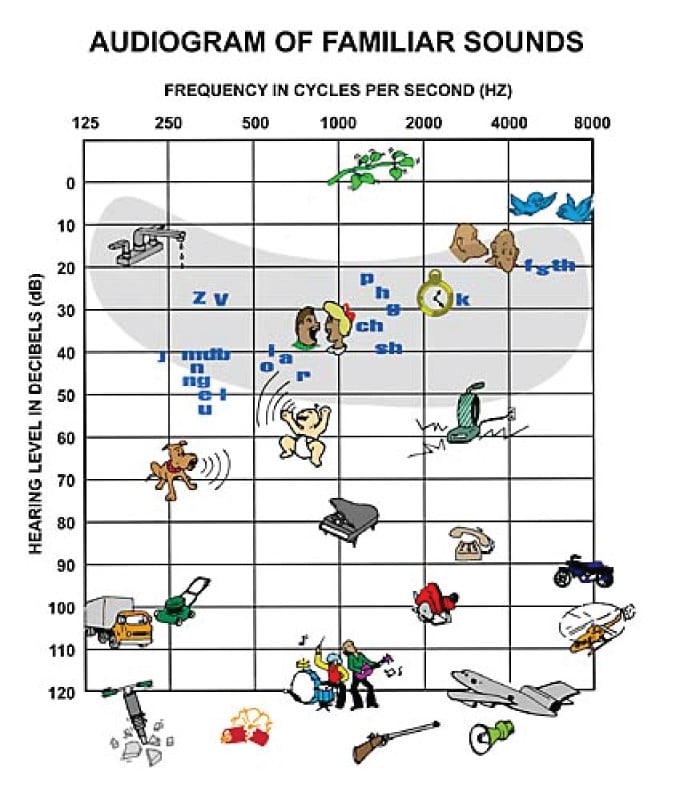
- Notice the frequencies
of familiar sounds of our environment compared to how loud these sounds usually
are in our day-to-day activities. For
instance, a loud rock and roll band is at 120 decibels. - Notice the
frequencies of individual speech sounds… f, s and th sounds are consonant
sounds of speech at the ‘higher’ frequency of 4,000 Hz and usually ‘quiet’
decibel level of 20 dB. - Notice the grey
shaded ‘speech banana’ that represents the frequency and hearing level for
normal human conversation. This speech
banana is what we compare to your own graph on the audiogram.
Audiogram: Levels of Hearing Loss
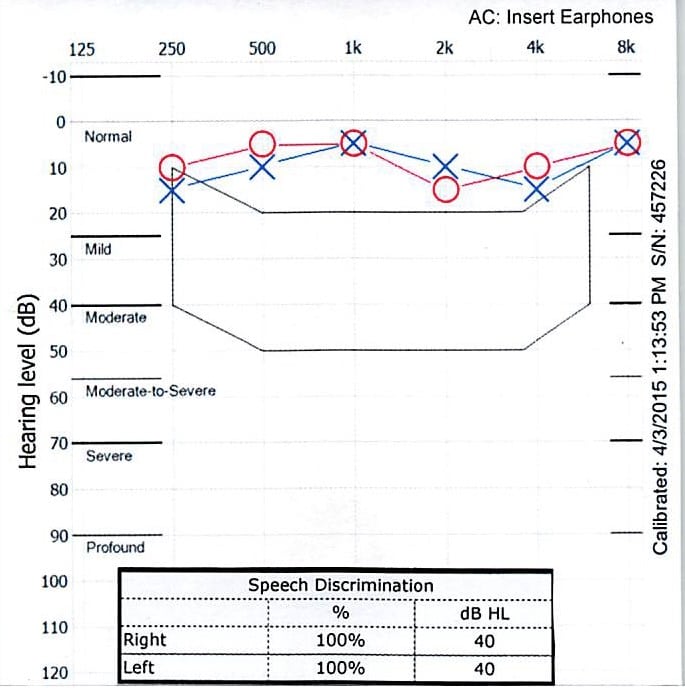
- This is an actual audiogram
from our office showing normal hearing.
Note the markings for the right ear (O) and the left ear (X). Again, it represents a graph of how loud the sounds and speech need to
be for you to be able to hear them for the individual frequencies of speech. 0 dB is ‘quiet’ and 120 dB is really loud; for
the frequencies, 125 is a low frequency sound (vowels), and 8,000 (8k) is a
really high frequency sound (consonants). - Also on this graph
is the ‘speech banana’ (irregular box shaped area) mentioned previously… this
is the range of normal conversation, for the most part between 20db and 50db
loudness. - The other important
addition to audiogram is the ‘Speech
Discrimination’. This is measure of
how well your brain understands
speech. It’s not a perfect test, as it
measures only the percent of words you understand in the quiet of a hearing
booth… it doesn’t measure what happens in the conversations of a party or in
the loud background noise of a restaurant. - Lastly, note the
markings of Normal, Mild, Moderate,
Moderate-to-Severe, Severe and Profound on the left side of the graft. These represent the ‘Levels of Hearing Loss’
present for everyday sounds and speech.
After the Audiologist completes your audiogram you will return back to my office to discuss your audiogram. The audiogram will likely show four possible patterns:
- Normal Hearing
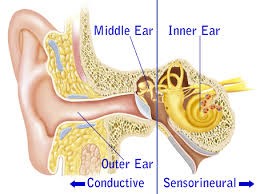
as shown by the first audiogram. - Problems with the outer/middle ear function, where the auditory canal, eardrum or
hearing bones are not able to effectively conduct sound to the inner ear. Reasons for this type of hearing loss
(conductive hearing loss) would be ear wax in the auditory canal, fluid behind
the eardrum, a perforation of the eardrum, or fixation of hearing bones from
scar tissue of recurring ear infections.
Most of these conditions can be managed by medications or surgery. - Problems with the inner ear function, where the inner ear
is not able to take the energy in a sound wave and create nerve energy for the
brain to use for understanding sound and speech. The most common reasons for this type of
hearing loss (sensorineural hearing loss) would be age, genetics, and excessive
noise exposure. This type of hearing loss can be improved by
the use of hearing aids. - A combination of
the last two… having both a conductive and sensorineural problem.
However, over 90% of the patients we see will have problems of the inner ear… usually due to the combined effects of aging, genetics and noise exposure. So, let’s take a look at a series of audiograms for this group of patients.
Along with the first normal audiogram, the following two audiograms show the ‘progression of hearing loss’ with the inner ear not able to hear sounds and the brain not able to understand human speech (Speech Discrimination).
I want to repeat two important points about the audiogram:
- The ability to
hear sounds is represented by the (O) marks for the right ear and the (X) marks
for the left ear. - The brain’s ability
to understand human speech is represented by the Speech Discrimination score, or the percent of words you understand
in the audio booth.
And remember, the Speech Discrimination score is not perfect… it doesn’t really accurately reflect what you are understanding in the noisy restaurant. I’ll come back to the brain issue after we look at the next two audiograms showing the ‘progression of hearing loss’ present in my family.
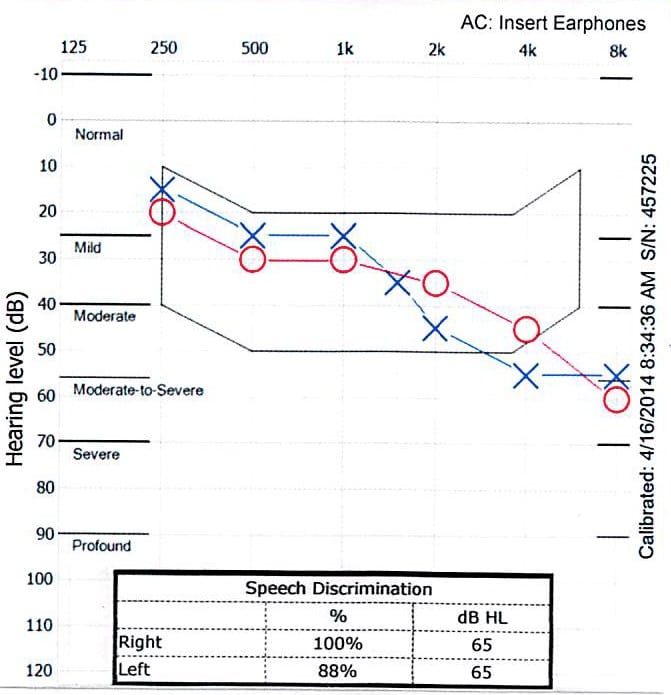
Mild/Moderate Hearing Loss
- This is my
audiogram at age 65. I have normal/mild
hearing loss in the lower frequencies and drop down to a moderate hearing loss
between 2,000 – 8,000 Hz. - I have problems in
groups, at parties, and restaurants; I
have to concentrate on facial expressions and ‘lip movements’ to understand
some conversations; I sometimes miss words even during one-on-one
conversations; I may commonly ask people to repeat themselves. - Notice that my
Speech Discrimination score was only 88% for the left ear. This means I’m starting to have ‘brain problems’
understanding speech.
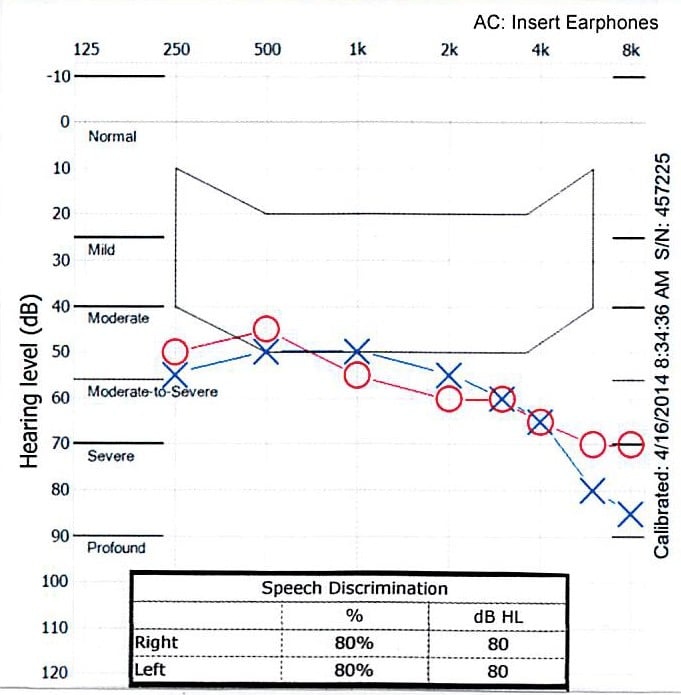
Moderate/Severe Hearing Loss
- This was my
mother’s audiogram at age 84… she had been wearing hearing aids for about 12
years. (Yes, part of my hearing issue is
genetic.) - Unless she was
wearing her hearing aids, she found it impossible to understand conversations
in groups or restaurants; telephone
conversations were difficult; unless she was wearing her hearing aids, she would
not even hear the doorbell ring. - Her Speech
Discrimination score was 80%… in the quiet of a hearing booth. It was a lot worse when there was the
background noise of a party or at a restaurant.
Hearing & The Brain
Five years ago, I produced my first article on hearing loss and how your ENT physician and audiologist team evaluate your hearing and then work towards improving hearing and quality of life. The article also introduced information on one aspect of hearing loss that was not widely appreciated – the association of age-related hearing loss (presbycusis) with dementia; dementia being described as an abnormal loss of memory and ability to think clearly (cognition). Since my last article there has been an ongoing push to better understand how hearing loss, cognition and dementia are related, as well as proving what seems to be common sense – how hearing aids can improve age related hearing loss, quality of life, and how to slow down or prevent dementia. To build on what I wrote five years ago I am going to add additional information from articles in the medical literature.
First, what is known about the association of hearing loss, cognition and dementia?
To paraphrase from articles written by Frank Lin MD, an ear specialist at Johns Hopkins University:
- Individuals with a
mild hearing loss have twice the risk of developing dementia; those with
moderate hearing loss have three times the risk of developing dementia; and
those with severe hearing loss have five times the risk of developing dementia. - Hearing impairment
is associated with a 30-40% rate of accelerated cognitive decline. - Hearing loss is
associated with a decrease in actual brain volume in the part of the brain
associated with hearing. - Hearing loss is
known to cause individuals to isolate themselves from family and friends. This loss of social engagement and resulting
depression is a major problem for those of us trying to maintain good health as
we age. - There are common
risk factors that impact both the cochlea of the ear and the brain. These would include age, vascular risk
factors such as high blood pressure, diabetes and smoking, and the level of
education and ability to compensate for loss of hearing and cognition. - Hearing loss may
be a thought of as a ‘second hit’ on the brain, with the overall effect of
hearing loss adding to the decrease in cognitive performance associated
with other brain problems such as Alzheimer’s and vascular risk factors.
Hearing loss is clearly ‘associated with dementia’. But, this is different than saying, ‘hearing loss causes dementia’. At this time, while hearing loss has not been shown to cause dementia, a 2017 article in The Lancet, titled ‘Dementia Prevention, Intervention and Care’, postulated that hearing loss was the largest ‘modifiable risk factor’ for dementia in patients over the age of 55. (Other modifiable risk factors are level of education, high blood pressure, obesity, smoking, depression, physical inactivity, social isolation, and diabetes.) One theory of aging and hearing research suggests that hearing loss makes the brain use its ‘cognitive reserves’ in its effort to understand the world around us. In other words, hearing loss makes our brain work extra hard to understand what is going on in our immediate surroundings. But as our brain does all this extra work associated with our hearing loss, we damage other brain functions such as memory and the ability to interact socially. The end result of combining hearing loss with aging and dementia is that we pull away from world – social isolation leading to depression, etc.
So… if hearing loss is the largest ‘modifiable risk factor’ – usually modified by the use of hearing aids – what current evidence is there that hearing aids improve cognitive function or decrease the risk of dementia?
- A University of
Michigan team published a 2016 article in the Journal of the American Geriatrics Society postulating that
older adults who get hearing aids for newly diagnosed hearing loss have a lower
risk of being diagnosed with dementia (18% lower), depression or anxiety (11%
lower), and a decrease in the risk for falls (13% lower) for at least the next
three years. - A 2015 British
study looked at, ‘Hearing Loss and Cognition: The Role of Hearing Aids, Social
Isolation and Depression”. Their
study postulated that hearing aid use was associated with better cognition, and
was independent of the effects of social isolation and depression. - Following the
Lancet study which postulated that hearing loss was the largest modifiable risk
factor for preventing dementia, a study titled, ‘Wearing Hearing Aids May
Protect Brain Later in Life’ came out of the University of Exeter. The group of patients who wore hearing
aids performed better in measures assessing working memory and aspects of being
able to pay attention than those who did not wear hearing aids. - Another
article showing only the association between hearing aids and improved
cognitive function, was “Self-Reported Hearing Loss: Hearing Aids and Cognitive
Decline in Elderly Adults: A 25-year Study”,published in the October edition of
the Journal of the American Geriatrics
Society. They compared the trajectory of cognitive
decline among older adults who were using hearing aids and those who were not. The
study found no difference in the rate of cognitive declinebetween people with no reported hearing loss and people with
hearing loss who used hearing aids. - Lastly, the
results of the ACHIEVE (Aging and Cognitive Health Evaluation in Elders) study
looking at hearing aid treatment for reducing cognitive decline is ongoing at
Johns Hopkins University (Drs Lin and Coresh).
Estimated time with results… sometime in 2022.
Call David Brown, M.D. Ear Nose & Throat PC for more information or to schedule an appointment.